
Ultimate Guide
to Endoscope
Reprocessing
Steps, Standards, and Best Practices for Infection Prevention in Every Endoscopy Setting
Why This Guide Matters
Endoscope reprocessing is one of the most critical infection prevention processes in any clinical setting. Unlike most reusable medical devices, flexible endoscopes cannot be steam-sterilized, making a precise, multi-step reprocessing protocol the only line of defense between contaminated instruments and patient safety.
This guide covers everything: from foundational definitions and regulatory frameworks, to step-by-step reprocessing workflows, department design, accessory selection, training standards, and the most common mistakes made in the field.
Whether you're a GI nurse, sterile processing technician, endoscopy manager, or facility administrator, this resource gives you the clinical authority and practical tools to build, evaluate, and improve your reprocessing program.
Download Resource PacketAll citations in this guide are marked with superscript numbers throughout the text. A complete Master Works Cited list appears at the end of the guide, consolidating all references in a single location.
Why Endoscope Reprocessing Matters
Every day, in hospitals, ambulatory surgery centers, and outpatient GI clinics across the United States, flexible endoscopes move from one patient to the next. They travel through the esophagus, stomach, colon, and bile ducts, collecting blood, mucus, tissue, and the full spectrum of a patient's gut flora along the way.
Before that same instrument enters the next patient's body, it must be thoroughly and correctly reprocessed. When that process works as intended, the risk of patient-to-patient infection transmission is vanishingly small. When it doesn't, the consequences can be deadly.
The sheer volume creates an environment where even a small rate of protocol deviation can translate into a significant number of patients put at risk. The stakes are not hypothetical. They are documented, reported, and in some cases, fatal.
What the FDA's Adverse
Event Data Tells Us
The FDA's MAUDE database is the most comprehensive public record of medical device-related adverse events in the country. A comprehensive analysis by Dr. Lawrence Muscarella, PhD, covering January 2014 through December 2021, reviewed more than 10,000 adverse event reports describing actual or potential contamination of a reprocessed flexible endoscope deemed "patient-ready."4
The types of events documented in MAUDE span the full range of reprocessing failure modes:
Contamination with Microorganisms & Biofilms
Scopes confirmed contaminated with microorganisms, patient fluids, or biofilms, all deemed ready for patient use at the time of the event.4
Equipment Failures
AERs with leaking disinfectant, clogged or long-overdue water filters, and malfunctioning cycle monitors, undetected during routine use.7
Unverifiable Reprocessing Cycles
Endoscopes reprocessed while the AER printer was non-functional, meaning cycle completion could not be verified.7
A facility's technician was observed using an AER without the required hookup connectors, while visible bioburden was present on the distal end of the scope and inside the suction valves.7
A facility applied oven cleaner to the basin of an AER, cracking and contaminating it, before a field engineer who happened to be on-site intervened.7
These are not rare-edge cases. They are the documented reality of what occurs in facilities where training, oversight, and strict IFU adherence are not consistently enforced.
The Duodenoscope Crisis:
A Watershed Moment
No single episode illustrates the stakes of endoscope reprocessing more clearly than the duodenoscope-associated CRE outbreaks that came to widespread attention between 2013 and 2016.
Duodenoscopes are used in ERCP, a critical procedure for diagnosing and treating pancreatic and biliary disorders. More than 500,000 ERCP procedures are performed annually in the United States.8 Their elevator mechanism and elevator channel proved extraordinarily difficult to clean, and the consequences were devastating.
By early 2015, a cluster of CRE infections at UCLA Medical Center made national news. The CDC confirmed that investigators found no recognized breach in reprocessing, underscoring that even careful protocol adherence may not fully eliminate the risk posed by the duodenoscope's complex design.10
The FDA issued a formal Safety Communication on February 19, 2015, acknowledging that infections might still occur even when the manufacturer's reprocessing instructions were followed correctly.8 The FDA simultaneously issued warning letters to Olympus, Fujifilm, and Pentax.8
"The FDA's regulatory system had failed to quickly identify and resolve the spread of duodenoscope-linked antibiotic-resistant infections, and that tragedies occurred which could have been prevented.", Senate Report11
This episode led to new FDA-mandated post-market surveillance studies, revised manufacturer IFU, and ultimately the FDA's endorsement of transitioning to disposable-cap and fully single-use duodenoscope designs.
The Human Cost
of Complacency
Behind every statistic and every adverse event report is a patient who trusted a healthcare facility with their safety.
Endoscopy patients are often already vulnerable, many are undergoing screening for cancer, managing chronic GI disease, or navigating complex biliary or pancreatic conditions. They consent to a procedure that they trust has been made safe by the systems and standards their healthcare team upholds.
For the patients who contracted CRE infections following ERCP, the consequences ranged from extended hospitalization and aggressive antibiotic therapy to, in documented cases, death.8,9
"The science is clear. The standards exist. The guidelines are published, endorsed by every major GI and infection control society, and updated regularly. What stands between safe patient care and preventable harm is the disciplined, consistent, step-by-step execution of the reprocessing protocol, every time, by every technician, on every scope."
Why Anatomy Is a Reprocessing Prerequisite
You cannot reliably clean something you do not understand. That principle is at the core of every professional certification in endoscope reprocessing, the HSPA's Certified Endoscope Reprocessor (CER) exam devotes an entire domain to "Endoscope Purpose, Design and Structure," explicitly testing knowledge of endoscope categories, anatomy and components, and the processing challenges related to each design.11 The reason for that emphasis is not academic: the physical architecture of an endoscope determines where contamination hides, which steps in reprocessing are most critical, what tools and brushes are required, and what level of disinfection or sterilization is appropriate.
The Basic Framework: How Endoscopes Are Classified
Endoscopes are broadly classified by two intersecting systems: their physical structure (rigid, semi-rigid, or flexible), and their intended clinical use and patient contact risk (which determines the required level of reprocessing under the Spaulding Classification). The HSPA CER exam content outline defines three primary structural categories.
Rigid endoscopes have a straight, inflexible metal tube and a fixed optical system. They cannot be bent. They enter the body through surgical incisions (laparoscopes, arthroscopes, thoracoscopes) or through natural orifices with minimal curvature (cystoscopes, sinuscopes, laryngoscopes). Their relatively simple, solid construction makes them compatible with steam sterilization, which is the gold standard for critical and semicritical devices.12
Semi-rigid endoscopes occupy the space between rigid and flexible with limited deflection capacity. Ureteroscopes are a common example. Semi-rigid instruments are less common than their counterparts at either end of the spectrum and are often discussed alongside rigid instruments in reprocessing literature.
Flexible endoscopes have a plastic and polymer insertion tube capable of bending around curves and navigating the tortuosity of the gastrointestinal tract, bronchial tree, or urinary system. Their flexibility is the feature that makes them indispensable for GI endoscopy, and also the feature that makes their reprocessing profoundly more complex than any other class of reusable medical device.13
By Clinical Use: The Spaulding Classification
The Spaulding Classification System, developed by Earle H. Spaulding in the 1950s and refined over subsequent decades, categorizes all patient-care items based on their infection risk.14
Critical Devices
Enter sterile tissue or the vascular system. They must be sterile before every use. Surgical instruments, biopsy forceps, and needles are examples.
Semi-Critical Devices
Contact mucous membranes or nonintact skin but do not ordinarily penetrate sterile tissue. They require at least high-level disinfection (HLD) after every use. Flexible GI endoscopes, bronchoscopes, and many rigid endoscopes fall into this category. When flexible endoscopes are used therapeutically, during polypectomy, biopsy, treatment of GI bleeding, instruments passed through the working channel penetrate the mucosal barrier, placing those accessories firmly in the critical category.14,15
Non-Critical Devices
Contact only intact skin or do not directly contact the patient. Low-level disinfection or cleaning is sufficient.
A Closer Look at Flexible Endoscopes
A flexible endoscope is one of the most complex reusable instruments in clinical medicine. Beneath its smooth polymer exterior lies an intricate system of optical pathways, angulation wires, multiple fluid channels, and delicate electronic components, all packed into a tube rarely wider than 12 millimeters in diameter.17 Understanding this internal architecture is not optional for reprocessing staff. It is prerequisite knowledge.
Every modern flexible videoscope is organized into three principal sections that must each be understood independently for proper handling, cleaning, and reprocessing.18
1. The Connector Section (Umbilical)
The connector section, sometimes called the universal cord or umbilical, is the proximal end of the endoscope that plugs into the external equipment stack: the light source, video processor, and water bottle. It contains the light guide connector (the only opening to the internal components), electrical connections for video signal transmission, and the suction port that connects to wall or portable suction.18,19
2. The Control Section (Control Body / Handle)
The control section is the operator's command interface, the part held in the endoscopist's left hand during a procedure. It is the most mechanically complex component of the scope that staff will handle directly during reprocessing, and it contains multiple surfaces, ports, and removable components that must each be addressed.18
Angulation knobs: Two concentric knobs connected internally to a system of pull-wires that run the entire length of the insertion tube to the distal bending section.
Suction valve and air/water valve: Removable for cleaning, and must be removed and cleaned individually at every reprocessing cycle. Valves cleaned while still attached to the scope represent a common reprocessing failure mode.19
Biopsy port (instrument channel port): The entry point for all accessories, biopsy forceps, snares, injection needles, hemostatic clips, polypectomy snares.
Remote switches: Programmable buttons for video processor control (image capture, freeze frame, contrast adjustments).
3. The Insertion Section
The insertion section is the long, flexible component that enters the patient's body. It is the most technically sophisticated part of the endoscope and the most important to understand for reprocessing purposes.
The bending section is located at the distal end of the insertion tube and is the zone of maximum angulation. It is covered with a soft rubber bending rubber that enables deflection of the tip up to 180-210 degrees in some scope models. The bending rubber is one of the most frequently damaged components on flexible endoscopes, cracks, tears, or perforations here represent a direct pathway for contamination to enter the internal components. It is a primary site for inspection during every leak test.
The distal tip is the "business end" of the endoscope, packing multiple systems into a capsule barely larger than a pencil eraser.20 It usually contains the lens and imaging sensor, light guide/system, air/water nozzle, and a biopsy channel.
Flexible endoscopes contain long, narrow channels that cannot be visually inspected, cannot be steam sterilized, and must be cleaned using brushes, flushing, and enzymatic detergents applied under specific mechanical conditions. Every channel has a specific brush size requirement, using the wrong brush means either failing to contact the channel walls (too small) or damaging the channel lining (too large).20
Flexible endoscopes emerge from GI procedures harboring contamination of a scale not associated with most surgical instruments. The internal compartments of intestinal endoscopes can contain up to 1020 enteric microbial cells.14 Under conditions where cleaning is delayed or inadequate, these organisms begin forming biofilm within the channels, a matrix that protects organisms from disinfectants and cleaning agents.18
Steam autoclaving is incompatible with flexible endoscopes, forcing reliance on HLD or low-temperature sterilization methods. Dr. William Rutala has described the reason for endoscope-related infection outbreaks as the minimal or nonexistent margin of safety associated with HLD of these instruments.16 Unlike sterilization, which achieves a Sterility Assurance Level of 10-6, HLD does not provide a quantified safety margin.
Reprocessing Standards & Regulations
Endoscope reprocessing does not operate in a regulatory vacuum. It sits at the intersection of clinical standards, federal oversight, accreditation requirements, and professional society guidance. For anyone running an endoscopy program, whether in a hospital, ambulatory surgery center (ASC), or outpatient GI clinic, understanding which organizations govern reprocessing, what authority each carries, and how their guidance layers together is foundational to building a defensible, compliant program.
ANSI/AAMI ST91:2021, The Comprehensive Operational Standard
The most technically detailed reprocessing standard in the U.S. is ANSI/AAMI ST91:2021, Flexible and Semi-Rigid Endoscope Processing in Health Care Facilities, published by the Association for the Advancement of Medical Instrumentation (AAMI) and released in March 2022. ST91 is the operational blueprint for reprocessing programs, it covers every stage from point-of-use treatment through storage, and governs facility design, water quality, staff training, equipment qualification, and quality control.40
Two-Room Design Requirement
A preferred two-room design for endoscope processing areas, with physical separation between decontamination and clean workrooms. Where two-room design is not immediately feasible, strict unidirectional workflow with at least four feet of separation between soiled and clean zones is required.40
Water Quality Monitoring
Cross-referenced to AAMI ST108:2023, with specific water quality parameters for each processing stage and required testing at point of generation and point of use.41
Cleaning Verification
Cleaning verification after each use of high-risk endoscopes, using rapid indicator tests (ATP, protein, or hemoglobin), with borescope inspection recommended for visualizing interior channel conditions.40
10-Minute Forced Air Drying
Minimum 10-minute forced air drying of all internal channels using pressure-regulated instrument air or HEPA-filtered air before storage.41
Training & Certification Requirement
A recommendation that all personnel performing endoscope processing duties complete formal training and competency verification before first solo assignment, and obtain professional certification within two years of employment.41
Hand-off Communication
From point of use to decontamination, including at minimum: patient identifier, date of procedure, time point-of-use treatment was completed, and employee contact.41
SGNA Standards, The Nursing and Associates Practice Standard
The Society of Gastroenterology Nurses and Associates (SGNA) publishes two foundational reprocessing documents that are the primary standard-of-practice reference for GI nursing staff and endoscopy technicians: the Standards of Infection Prevention in Reprocessing of Flexible Gastrointestinal Endoscopes (2018, with periodic updates), the nine-step reprocessing sequence used as the operational reference throughout the GI endoscopy nursing community, and the Standard of Infection Prevention in the Gastroenterology Setting (2019).42 SGNA's guidance on precleaning timing, brush selection, valve handling, MEC testing, and storage is authoritative for every accreditation survey a GI facility will face.
ASGE/SHEA Multisociety Guideline, The Evidence-Based Clinical Framework
The Multisociety Guideline on Reprocessing Flexible GI Endoscopes and Accessories (2021), developed by the ASGE Quality Assurance in Endoscopy Committee with co-sponsorship from SHEA, ACG, AGA, and AASLD, provides the evidence-based clinical backbone for reprocessing programs.43 It uses the GRADE methodology to rate the strength and quality of evidence behind each recommendation and critically examines four unresolved questions: whether repeat HLD reduces contamination compared to single HLD; whether ethylene oxide sterilization reduces contamination compared to single HLD; what the maximum safe endoscope storage time is; and what the efficacy of microbiologic surveillance is in detecting contamination.
2025 SHEA Multisociety Guidance, The Most Current Update
In April 2025, the Society for Healthcare Epidemiology of America (SHEA) published new multi-society guidance on sterilization and HLD of reusable medical devices, including lumened endoscopes, in partnership with ASGE, SGNA, APIC, AAMI, AORN, HSPA, and IDSA.44 This guidance follows the 2024 update of the CDC/HICPAC Guideline for Disinfection and Sterilization in Healthcare Facilities and represents the most current authoritative framework for reprocessing practice. Every facility performing GI endoscopy should review this guidance and reconcile it with their current policies.
CDC/HICPAC Guideline
Originally published in 2008 and substantially updated in 2024, provides the federal-level framework for disinfection and sterilization of all reusable medical devices. The CDC does not enforce compliance directly, but its guideline is foundational to accreditation standards.45
FDA
The FDA has authority over endoscope manufacturers, not directly over healthcare facilities, but its actions fundamentally shape reprocessing practice through Manufacturer IFU clearance, Safety Communications and Warning Letters, the MAUDE database, MedWatch, and High-Level Disinfectant Clearance. Resources at fda.gov/medical-devices/reprocessing-reusable-medical-devices.
The Joint Commission & CMS
The Joint Commission surveys hospitals and ASCs against a standards framework that incorporates reprocessing requirements. Non-compliance can trigger citations, corrective action requirements, and in serious cases, threatens accreditation.
AORN
Publishes its Guideline for Processing Flexible Endoscopes as part of its perioperative standards library. AORN's 2022 guideline update aligns with ST91 on the 10-minute forced air drying requirement and two-room design preference.47
APIC & IDSA
Both contributed to the 2025 SHEA guidance and provide infection prevention expertise applicable to reprocessing programs. APIC's infection preventionists are a key resource for facilities responding to reprocessing failures, developing surveillance programs, and managing outbreak investigations.44
Scope-Specific IFU
Every flexible endoscope manufacturer produces model-specific Instructions for Use validated for that specific instrument. IFUs specify brush sizes, cleaning adapters, approved disinfectants, leak testing procedures, water temperatures, storage requirements, and repair instructions. Deviating from IFU constitutes a compliance gap regardless of other standards followed.
Every endoscope reprocessing program should maintain a current copy of each of these primary documents and designate a responsible person, typically a GI nurse manager, infection preventionist, or sterile processing director, to monitor and implement updates as they are published.
The Nine-Step
Reprocessing Standard
The SGNA's Standards of Infection Prevention in Reprocessing of Flexible Gastrointestinal Endoscopes defines nine sequential steps that form the operational backbone of every GI endoscope reprocessing protocol.42 These nine steps are also reflected in the ASGE Multisociety Guideline, ANSI/AAMI ST91:2021, and the CDC/HICPAC guideline.
They are not interchangeable in order. Each step depends on the successful completion of the step before it, and no step can be skipped without compromising the integrity of all subsequent steps.
Always reference device and endoscope IFU for specific cleaning steps.
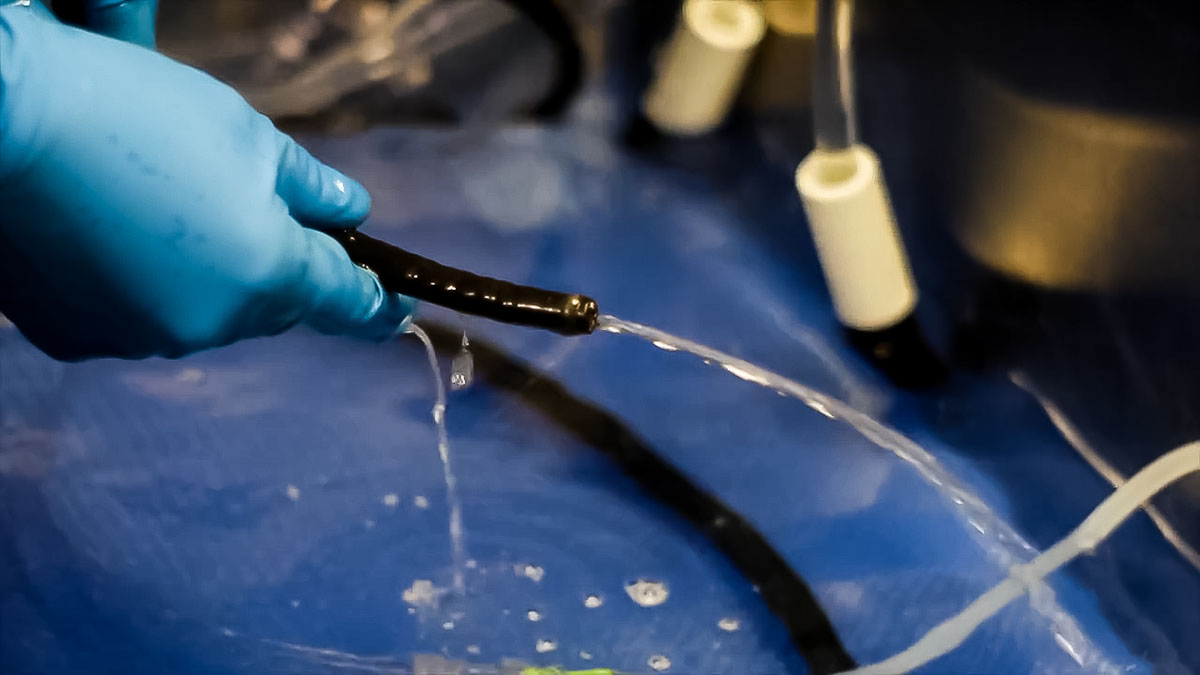
Point-of-Use
Pre-Cleaning
Why it's critical: Pre-cleaning begins the process of removing bioburden before it dries and becomes dramatically harder to remove. A flexible endoscope used in a GI procedure can harbor billions of microorganisms; allowing patient secretions to dry inside channels initiates biofilm formation and increases the microbial load that subsequent manual cleaning must overcome.48
Wipe the external surface of the insertion tube with a soft, lint-free cloth dampened with an approved detergent or enzymatic solution, wiping from the control body toward the distal tip.
Place the insertion tube into a basin of fresh, diluted enzymatic detergent solution prepared according to the manufacturer's instructions.
Activate suction to draw the detergent through the suction/biopsy channel until the fluid runs clear.
Flush the air/water channel using the air/water cleaning adapter per the manufacturer's IFU.
Cap or plug the scope per IFU for transport.
Transport immediately in a fully closed, puncture-resistant, leak-proof, biohazard-labeled container to the reprocessing area.
Hand-off communication accompanying the scope must include at minimum: patient identifier, date of procedure, time pre-cleaning was completed, and employee contact.41
Delayed pre-cleaning. Manufacturer IFUs specify a maximum time window for completing pre-cleaning after a procedure, this window must be followed.

Leak
Testing
Why it's critical: A leak test confirms the structural integrity of the scope's internal components. If a scope with an internal leak is immersed without a leak tester maintaining positive internal pressure, fluid can enter the sealed compartments housing electronics, optics, and angulation components, causing catastrophic and expensive damage.49
Attach the leak tester to the leak test port per the manufacturer's IFU.
Perform a dry leak test first: apply the recommended positive pressure and confirm it holds for the specified duration without visible deflection.
Perform a wet leak test: with positive pressure maintained, immerse the scope in clean water and observe for a continuous stream of bubbles. Note: single bubbles at angulation rubber are common; sustained streams indicate a true leak.
If no leak is detected, proceed. Maintain positive pressure throughout subsequent manual cleaning steps per manufacturer IFU.
If a leak is detected, keep positive pressure applied (to prevent fluid ingress), remove the scope from service, and follow the facility's damaged scope policy.
Automated leak testers must be placed on a calibration schedule, and pressure verification must be performed on every day endoscopes are used.41 Mechanical leak testing through an AER is not a substitute for manufacturer-IFU-specified leak testing.
Performing leak testing after AER rather than before, a commonly observed error that means any internal damage has already been exposed to harsh chemicals.

Manual
Cleaning
Why it's critical: The SGNA explicitly states that manual cleaning "is the most critical step in removing the microbial burden from an endoscope. It requires focused and deliberate attention."42 Disinfectants cannot penetrate organic soil, protein deposits, or biofilm. If cleaning is incomplete, HLD cannot achieve its intended outcome, period.
Prepare fresh enzymatic detergent solution at the manufacturer's specified temperature and concentration. Never reuse enzymatic solution.
Fully submerge the scope in the basin.
Wipe all external surfaces, including the insertion tube, control body, and umbilical cord, with a soft cloth.
Remove, disassemble, and individually clean all removable components (suction valve, air/water valve, biopsy port cap/valve).
Using the correct brush size per the IFU for each specific scope model, brush all accessible channels: insert the brush into the biopsy port, advance the full length until the brush emerges at the distal tip, then withdraw. Repeat until the brush emerges clean.
For duodenoscopes: repeatedly raise and lower the elevator throughout brushing to expose the elevator recess area. Use the specific brushes required for the elevator wire channel per the manufacturer's updated IFU.
Flush all channels, including air, water, and suction/biopsy, using the appropriate channel-specific flushing adapters, per IFU. Channels too small to brush must still be flushed.
Rinse all surfaces and channels thoroughly with clean water to remove all detergent residue.
Using the wrong brush size (too small = insufficient wall contact; too large = channel damage); reusing enzymatic solution; skipping the elevator channel on duodenoscopes; inadequate flushing of air/water channels.

Rinse After
Manual Cleaning
Why it's critical: Residual enzymatic detergent must be completely removed before HLD. Detergent residue can interfere with the activity of some high-level disinfectants and may cause chemical injury to patients if introduced into the body cavity.
Thoroughly rinse all external surfaces and flush all internal channels with clean water until no residual soap, foam, or detergent odor remains. Use the channel flushing adapters per manufacturer IFU.
Once rinsing is complete, the scope moves to visual inspection and cleaning verification, the gate that determines whether HLD can proceed. This step is often rushed and is a significant source of downstream failure.
Visual Inspection &
Cleaning Verification
Why it's critical: Visual inspection identifies damage and any visible residual soil before disinfection proceeds. Cleaning verification adds objective testing where visual inspection alone is insufficient.
Inspect all external surfaces under adequate lighting for cracks, tears, abrasion, discoloration, or physical damage.
Inspect the bending rubber, distal tip, and biopsy channel inlet for damage, tears, or foreign material.
Per ANSI/AAMI ST91:2021, cleaning verification (CV) tests, using rapid indicator tests for residual ATP, protein, or hemoglobin, are recommended after each use of high-risk endoscopes (duodenoscopes, echoendoscopes).41
Borescope inspection of internal working channels is recommended for periodic quality assurance and following any suspected damage event.41
If visible soil remains, return to manual cleaning. If structural damage is found, remove from service and follow facility policy for scope repair.
Assuming visual inspection alone is sufficient. Studies have consistently shown that endoscopes with residue detected via cleaning verification indicator tests can appear clean on visual inspection alone.50
High-Level
Disinfection
Why it's critical: HLD eliminates vegetative organisms, viruses, fungi, and most bacteria (but not all bacterial spores). It is the minimum standard of care for flexible GI endoscopes under the Spaulding Classification.45
Prepare HLD solution in a dedicated, covered basin per the manufacturer's instructions.
Test the solution concentration using the specific test strips approved for that disinfectant. Compare to the MEC or MRC. If below MEC, discard and prepare fresh solution, never use below-MEC solution.
Fully immerse the scope and attach all required channel connectors. Fill all channels completely with HLD solution.
Cover the basin and observe the full exposure time specified in the HLD manufacturer's label claim.
Document: disinfectant lot number, MEC test result, exposure time start and end, technician name.
Load the scope into the AER per both the AER manufacturer's IFU and the endoscope manufacturer's IFU. Use only approved connectors, incompatible or missing connectors mean channels are not exposed to disinfectant.
Confirm the correct AER cycle is selected for the scope model and HLD agent being used.
Run a complete cycle. If interrupted, the full cycle must be repeated.
Verify cycle completion per the AER documentation/printout. Document the cycle result.
Testing MEC with expired test strips; using below-MEC solution; running a partial AER cycle; using wrong connector; failing to verify cycle completion.

Rinse
After HLD
Why it's critical: Residual high-level disinfectant, particularly glutaraldehyde and OPA, can cause chemical colitis, mucosal irritation, or allergic reactions if introduced into a patient's body cavity. Thorough rinsing is mandatory.
Flush all internal channels with sterile water (or water meeting the quality requirements in the manufacturer's IFU) using the appropriate adapters. Rinse all external surfaces.
The water used for post-HLD rinsing must meet quality specifications. Tap water may introduce waterborne organisms at this stage and is not appropriate unless specifically permitted by the scope manufacturer's IFU.
Drying
Why it's critical: Residual moisture inside endoscope channels is the leading single factor in post-reprocessing contamination. Pseudomonas aeruginosa, Acinetobacter, and other waterborne pathogens can multiply from a few organisms to millions of colony-forming units within hours in a moist channel environment.51
Dry the external surfaces completely with a clean, lint-free cloth.
Using pressure-regulated, filtered instrument air or HEPA-filtered air, flush all internal channels for a minimum of 10 minutes per ANSI/AAMI ST91:2021.41
Do not rely on hanging alone for channel drying, vertical hanging without active air flushing is not an effective drying method for internal channels.43
Per many manufacturer IFUs, flush channels with 70-90% isopropyl alcohol before the forced air step. Note: there is evolving evidence on alcohol flushing benefit; facilities should review current evidence and their specific manufacturer IFU.52
Reattach no valves or caps after drying, these trap moisture.
ANSI/AAMI ST91:2021 specifies a minimum of 10 minutes of forced air flushing through all internal channels.41 This is a floor, not a target, drying cabinets with HEPA-filtered continuous airflow represent best practice and extend effective drying through the storage period.

Storage
Why it's critical: Improper storage re-contaminates a properly reprocessed scope. The goal is to store in conditions that maintain dryness, prevent physical damage, and protect from environmental contamination until the scope is needed for the next patient.
Store endoscopes in a closed, clean storage cabinet in a secure location, not in procedure rooms. Cabinets should be at least three feet from any sink.41
Hang scopes vertically (preferred) or in the orientation specified by the cabinet manufacturer. Do not coil, allow acute angulations, or allow scopes to touch the bottom of the cabinet or each other.
Store without valves or caps attached, these create moisture traps.
Label each scope with the date it was last reprocessed and its hang-time expiration per facility policy.
Inspect scopes before storage and again when retrieved for patient use.
Clean storage cabinets per manufacturer IFU, at minimum weekly, and whenever visibly soiled.
The SGNA recommends a maximum hang time of seven days based on supporting literature and risk assessment principles.53
The ASGE Multisociety Guideline notes that data are insufficient to specify a universal maximum, and directs facilities to develop site-specific policies based on a formal risk assessment.43 Studies have demonstrated safe hang times ranging from 7 to 21 days under optimal conditions; the 7-day SGNA recommendation is the most widely applied clinical standard in U.S. practice.

Department Design Considerations for Endoscope Reprocessing
Why Physical Design Is a Patient Safety Issue
The physical design of an endoscope reprocessing area is not a facilities management question, it is a patient safety and infection control imperative. A poorly designed reprocessing environment makes protocol adherence difficult, creates cross-contamination risk, exposes staff to chemical hazards, and undermines every clinical standard discussed in this guide. ANSI/AAMI ST91:2021 made significant updates to its design requirements, and facilities planning any renovation or new construction should treat this standard as the architectural mandate for endoscope reprocessing areas.40
The Core Design Principle: Unidirectional Flow
The foundational principle of reprocessing area design is unidirectional workflow: soiled instruments enter on one end, move sequentially through decontamination and disinfection stages, and exit on the clean end. At no point should clean endoscopes cross paths with soiled ones. Cross-contamination between a freshly processed scope and a contaminated incoming scope represents a complete failure of the reprocessing system, and a physical layout that requires staff to navigate around this risk introduces avoidable human error into every reprocessing cycle.
ST91:2021 recommends the two-room design as the preferred standard:40
Room 1: Decontamination / Soiled Side
Receives soiled scopes from the procedure area. Pre-cleaning assessment, leak testing, manual cleaning, and rinsing are performed here. Negative pressure relative to adjacent clean areas is ideal to contain aerosols and vapors.
Room 2: Clean Workroom / Clean Side
AER disinfection or manual HLD, post-HLD rinsing, drying, and scope storage occur here.
Ideally, a pass-through window or door, and in some configurations, a pass-through AER, allows scopes to transition from the soiled to clean side without staff carrying them through shared corridors.54 Where two-room design is not currently achievable, ST91:2021 states that "strict unidirectional processing procedures should be in place to reduce risks of cross-contamination" with a minimum of four feet of separation between soiled and clean work zones.40
Environmental Requirements
Ventilation and Air Handling
Reprocessing areas must be designed to protect staff from chemical vapors (particularly glutaraldehyde, OPA, and peracetic acid) and from bioaerosols generated during manual cleaning. ST91:2021 requires that HVAC systems comply with ANSI/ASHRAE/ASHE Standard 170, with negative pressure in the decontamination area relative to adjacent spaces.40
The decontamination area should maintain negative pressure relative to the clean workroom and corridors to prevent chemical vapor and bioaerosol migration.
Chemical vapors must not exceed allowable exposure limits. HLD agents should be handled in covered basins or under local exhaust ventilation where required.
Eyewash stations must be accessible to all reprocessing staff working with caustic chemicals, this is a non-negotiable safety requirement under OSHA standards and endorsed by the ASGE Multisociety Guideline.43
Temperature and humidity should be regulated per facility HVAC standards.
Water Quality and Plumbing
Water quality is an underappreciated reprocessing variable with direct patient safety implications. Post-HLD rinse water that is microbiologically contaminated can introduce waterborne organisms into a freshly disinfected scope, eliminating the benefit of HLD entirely. ANSI/AAMI ST91:2021 cross-references AAMI ST108:2023 for water quality standards, which include specific microbial quality parameters for utility water and critical water at each processing stage.40
Dedicated plumbing and drains for the reprocessing area, separate from patient care areas.
Water supply quality must be monitored and controlled at the endoscope processing sinks and all equipment.
Post-HLD rinsing typically requires water meeting "critical water" quality specifications per manufacturer IFU, facilities should confirm what their scope manufacturers require.
Following major repairs or changes to the water utility system, requalification testing must be performed before resuming use.41
Sinks and Workspace
Sinks in the decontamination area should be large enough to fully submerge the longest endoscope in the facility's inventory.
Storage cabinets must be located at least three feet from any sink to prevent splash contamination of stored clean scopes.41
Work surfaces should be cleanable, impervious, and durable, they will be in contact with enzymatic solutions, disinfectants, and scope materials.
All areas should be clearly labeled: "Soiled Instruments" and "Clean Instruments" zones must be visually distinct.
Storage Cabinet Selection and Maintenance
Storage cabinets are a critical final step in the reprocessing chain. Options range from passive ventilated cabinets to active forced-air drying cabinets. Evidence supports the superiority of active drying cabinets in achieving complete channel drying, one study found active cabinets shortened external drying from 24 hours to 3 hours and internal channel drying from over 24 hours to approximately one hour.52
Adequate height to accommodate the longest scope in inventory without coiling.
Forced-air capability if serving as drying cabinet (per ST91:2021 recommendation for active drying).
Cleanable interior surfaces, with clear doors to minimize unnecessary opening.
Capacity for tracking/labeling individual scopes.
Lockable, located in clean, secure area, not in procedure rooms.
Common Mistakes when Reprocessing Endoscopes
The Documented Failure Modes
Understanding where reprocessing fails is as important as knowing the steps themselves. The literature consistently identifies the same categories of failures across outbreak investigations, audit studies, and adverse event reports. A Joint Commission review found 65.58% of hospitals non-compliant with sterilization and HLD standards, meaning the majority of facilities surveyed had at least one identifiable gap.46
Proper reprocessing of endoscopes can involve 50 to 100 discrete steps, and research shows that human error accounts for the majority of identified fail points.57
Pre-Cleaning and Transport Failures
Delayed or skipped pre-cleaning is one of the most consequential early errors. When bioburden is allowed to dry in channels before transport and manual cleaning, the result is dried protein deposits that resist enzymatic and mechanical removal. This directly undermines every downstream step. Improper transport containers, open bins, containers without biohazard labeling, containers that allow scope damage during transit, represent both a contamination risk and an OSHA Bloodborne Pathogen Standard violation. Missing hand-off communication means the reprocessing technician does not know when pre-cleaning was completed, creating uncertainty about whether the scope is within the manufacturer's acceptable pre-cleaning window.
Leak Testing Failures
Performing leak testing after the AER cycle instead of before is a widely documented error with serious consequences: the scope has already been immersed in enzymatic solution and high-level disinfectant, potentially flooding damaged internal compartments.49 Additional errors include not attaching the leak tester correctly per IFU; not maintaining positive pressure throughout the manual cleaning steps after a successful leak test; failing to calibrate or verify pressure on automated leak testers; and continuing to use a scope after a failed leak test (before repair).
Manual Cleaning Failures
Manual cleaning failures are the most clinically consequential category because cleaning is the foundational step upon which disinfection depends. Using the wrong brush size, insufficient brush passes, failure to clean all accessible channels, reusing enzymatic detergent solution, inadequate immersion time, and using off-label cleaning products or brushes are all documented and consequential failure modes. The elevator channel and recess of duodenoscopes require specific brushing steps that are frequently omitted.
HLD Failures
Using expired HLD test strips to verify MEC; using below-MEC disinfectant; incorrect AER connector hookup; interrupted AER cycle not restarted; and AER maintenance neglect (clogged filters, overdue water filter replacements) are all documented MAUDE adverse event failure modes.58 One MAUDE report described a facility that had not changed a water filter since 2019.
Drying and Storage Failures
Incomplete drying before storage is the most common single contributor to waterborne pathogen outbreaks post-reprocessing. Research found that 95% of stored, patient-ready scopes in one study retained residual liquid after automated reprocessing.57 Hanging scopes with valves attached, storing scopes in procedure rooms, and exceeding facility hang-time policy are among the most common storage errors.
Documentation and Quality Monitoring Failures
A 2022 case study of a urology practice found that among the most common compliance failures were: absence of precleaning documentation, improper documentation of materials and time periods for processing steps, and lack of training documentation for reprocessing staff.46 Documentation failures make protocol breaches invisible and traceability impossible when adverse events occur. The patient-scope traceability link is a fundamental requirement: every endoscope used on every patient must be documented in a format that allows retrospective identification of all patients exposed to a specific scope.
Human Factors
The endoscopy literature consistently identifies human factors, not equipment failures, as the primary driver of reprocessing errors. Staff fatigue, inadequate training on new scope models, use of temporary staff without competency verification, and normalization of deviation (when shortcuts occur without immediate visible consequences and become normalized practice) are all documented contributors to reprocessing failures.59 SGNA and ASGE both specify that temporary personnel should not be permitted to reprocess endoscopes until competency has been established and verified.42,43
Training, Competency, and Education
Endoscope reprocessing is among the most technically demanding infection control activities in healthcare. It involves up to 100 discrete steps; requires model-specific knowledge for every scope in a facility's inventory; uses chemical agents that can harm staff and patients if mishandled; and carries direct patient safety consequences when performed incorrectly. It cannot be learned adequately by observation alone or by reading a policy document.
Yet historically, many endoscopy units have trained reprocessing staff informally, a few days of observation followed by independent practice, with annual in-services that amount to a brief reminder. That approach is no longer consistent with professional standards, and accreditors are increasingly treating inadequate training documentation as a direct citation risk.
Regulatory and Guideline Requirements for Training
ANSI/AAMI ST91:2021 requires:40
All personnel performing endoscope processing duties must complete formal training and competency verification in all aspects of endoscope processing prior to their first solo assignment.
Competency must be verified for each specific endoscope make and model, equipment, equipment connections, and cleaning verification procedures, not just for "flexible endoscopes" generically.
Employees who process endoscopes should earn a professional certification in flexible endoscope processing within two years of employment and maintain that certification.
Temporary personnel should not be permitted to reprocess endoscopes until competency has been established and verified.
ASGE Multisociety Guideline requires:43
Competency evaluation of all reprocessing personnel performed and documented on a defined schedule: at commencement of employment, at least annually, whenever a breach is identified, when a major technique change or new endoscope model is introduced, and in the context of quality control efforts.
SGNA Standards require:42
Orientation programs and ongoing education structured for infection prevention and patient safety.
All healthcare workers, physicians, nurses, and assistive personnel, must be educated on appropriate infection prevention measures.
Competency should be assessed using auditing tools embedded in the training curriculum.
Certification Pathways
Requires a minimum of three months of hands-on experience reprocessing endoscopes and passing a 150-question computer-based examination. The exam content outline (updated 2023) covers seven domains: microbiology and infection control; endoscope purpose, design, and structure; work area design; workflow and processing steps; endoscope handling, transport, and storage; tracking, repair, and system maintenance; and human factors.60 Annual recertification through continuing education is required.
Requires 12 months of full-time flexible endoscope reprocessing experience (or an approved endoscopy technician course plus 6 months of experience). The exam covers accessories for endoscopic procedures, handling and cleaning of scopes and accessories, reprocessing of scopes and accessories, documentation, and ethics. Five-year recertification through continuing education is required.61
SGNA's GTS program is a recognition credential, not an exam-based certification, for GI associates and technicians. It is based on completion of SGNA's associates e-learning modules and is positioned as foundational education rather than an advanced certification. It is most appropriate as a first-step credential for new reprocessing staff early in their career development.62
Building & Auditing Your Reprocessing Program
A reprocessing program is not a policy document, it is an operational system. The policy is one component of the system, but it is only as good as the training, monitoring, documentation, and feedback mechanisms that support it. Building a durable reprocessing program requires attention to all of these elements simultaneously.
Written Policies and Procedures
Every endoscopy facility must maintain written reprocessing policies and procedures that reflect the current SGNA, ST91, and ASGE/SHEA multisociety guidelines; all manufacturer IFUs for every scope model and AER in use; facility-specific protocols for hang time, scope storage, chemical management, damaged scope handling, AER maintenance, and staff training; and response protocols for reprocessing failures including patient notification criteria. Policies should be reviewed and updated annually, and whenever new guidelines, manufacturer safety communications, or regulatory requirements are published.
Quality Monitoring and Documentation
Chemical Monitoring
MEC/MRC test strip results for every HLD cycle must be logged, with the date, technician name, disinfectant lot number, and pass/fail result. Test strip expiration dates must be checked on every shift, using expired strips is a documented and consequential failure mode. AER maintenance logs, filter change records, and chemical concentration logs should be maintained and accessible for survey.
Scope Tracking and Traceability
A scope tracking system must link every scope (by scope ID/serial number) to every patient on whom it was used, and to the reprocessing cycle completed after each use. Tracking must be sufficient to enable a complete patient notification list within 24 hours if an outbreak investigation is initiated.
Cleaning Verification Monitoring
Per ANSI/AAMI ST91:2021, cleaning verification (CV) testing should be performed after each use of high-risk endoscopes. CV results should be logged with scope ID, date, and technician. Failed CV results should trigger return to manual cleaning and investigation of the failure cause.
Microbiological Surveillance
Routine microbiological surveillance of reprocessed endoscopes is not universally required, but the ASGE Multisociety Guideline notes it can serve as part of a quality assurance program, particularly for duodenoscopes in ERCP settings.43 The FDA/CDC/ASM Duodenoscope Surveillance Sampling and Culturing Protocols provide standardized methodology for duodenoscope surveillance.
The Reprocessing Audit
Scheduled and unannounced audits of the reprocessing process are one of the most effective tools for identifying compliance gaps before they result in patient harm. The HICPAC Scope Reprocessing Audit Tool and the AmSurg Scope Reprocessing Audit Tool provide freely available frameworks that can be customized to facility needs.
An effective audit should be conducted by direct observation of actual reprocessing (not chart review alone), cover every step from pre-cleaning through storage, document findings with specific deficiencies (not just pass/fail totals), and generate a corrective action plan for every identified deficiency with a responsible person and target completion date. The ASGE Multisociety Guideline specifies that competency evaluation should be performed at commencement of employment, at least annually, and anytime a breach is identified.43 Many infection control experts recommend quarterly audits for high-volume units and at minimum semi-annual audits for lower-volume facilities.
Responding to a Reprocessing Failure
When a reprocessing breach is identified, whether through audit, surveillance culture, staff report, or patient adverse event, the response framework matters as much as the investigation.
1. Identify and quarantine all potentially affected endoscopes.
2. Conduct a preliminary review of reprocessing records for the affected scope(s) and timeframe.
3. Notify the facility's infection preventionist (IP) and relevant clinical leadership.
4. Assess the risk to any patients who may have been exposed to an inadequately reprocessed scope, in consultation with the IP and, where indicated, state/local public health.
1. Conduct a root cause analysis to identify which step(s) failed, why, and what systemic factors contributed.
2. Review documentation to determine the scope and duration of potential exposure.
3. Determine whether patient notification is required per state law, accreditor requirements, and CDC/HICPAC risk assessment guidance.
1. If the breach involved a device failure (AER malfunction, scope defect), report to the FDA MedWatch adverse event reporting system.
2. Report to relevant accreditation organization per their requirements.
3. If patient notification is required, coordinate with public health and legal counsel.
1. Implement targeted retraining for identified staff gaps.
2. Update written policies to address identified system gaps.
3. Conduct follow-up audit within 30--60 days to verify effective correction.
The Non-Negotiables: 10 Things Every Endoscopy Unit Should Do Today
These are the practices that, if not currently in place, represent the highest-priority gaps to address. They are drawn from the SGNA standards, ASGE Multisociety Guideline, ST91:2021, and the CDC/HICPAC Guideline, these are strong recommendations with supporting evidence, not optional enhancements.
Start pre-cleaning at the bedside, every time, within seconds of scope withdrawal.
There is no acceptable reason to delay this step. Establish a culture where pre-cleaning is as automatic as removing PPE after a procedure.
Perform leak testing before every immersion, before the scope touches cleaning solution.
Post-AER leak testing is a documented, consequential error. The protocol is fixed: leak test first, then immerse. No exceptions.
Use the correct brush for every channel in every scope model.
Post the manufacturer's brush size specifications at every reprocessing station. Do not allow improvisation.
Never reuse enzymatic detergent solution.
Single-use only. Fresh solution per scope, per cycle.
Test MEC before every HLD cycle and document the result.
Check test strip expiration dates at the start of every shift. A log without recorded results is not a log, it is a liability.
Complete channel drying with forced instrument air for a minimum of 10 minutes before storage.
Vertical hanging alone is not channel drying. Budget the time for proper drying before storing.
Store scopes without valves, without touching other scopes or cabinet floors, in closed, clean cabinets.
This takes 30 extra seconds and directly impacts the safety of the next patient.
Implement and enforce hang-time tracking for every stored scope.
If a scope's hang-time expiration is unknown when you reach for it, it must be reprocessed before use.
Document every reprocessing step, every scope, every cycle, with technician name and time.
Traceability is not paperwork overhead. It is the only way to respond to a patient safety event.
Verify, document, and re-verify staff competency, including for each specific scope model.
Competency verification is a regulatory requirement and a patient safety imperative. It is not optional for temporary staff, new employees, or staff assigned to scope models they have not been trained on.
FAQs: Common Questions Regarding Endoscope Reprocessing
Conclusion
Endoscope reprocessing is not a back-of-house administrative function. It is one of the most consequential patient safety practices in all of healthcare, and it happens in every endoscopy unit, every day, dozens of times per day, largely out of sight of the patients whose lives depend on it being done correctly.
This guide has covered the full arc of the discipline: the epidemiological and regulatory stakes, the anatomy of the instruments themselves, the authoritative standards and who enforces them, the nine-step reprocessing sequence that every technician must execute with precision, the physical and operational design of reprocessing environments, the special considerations that apply to high-risk instruments like duodenoscopes, and the training and auditing frameworks that keep programs defensible and effective over time.
Several themes run through every section of this guide, and they are worth naming clearly as parting thoughts.
Cleaning Is the Foundation
High-level disinfection and sterilization are powerful tools, but they are only as effective as the manual cleaning that precedes them. No AER, no chemical agent, and no automated system can compensate for a scope that was not thoroughly brushed, flushed, and inspected before disinfection began. This is the single most important operational principle in endoscope reprocessing.
Protocol Adherence Is Not Optional
Every documented case of healthcare-associated infection linked to a GI endoscope, in the absence of a device defect, has been traced to a breach in at least one reprocessing step. The protocol works when followed completely. The risk arises in the gaps, shortcuts, and normalized deviations that accumulate in high-volume, under-resourced, or inadequately trained environments.
Standards Require Active Management
The publication of ANSI/AAMI ST91:2021, the 2025 SHEA multisociety guidance, and ongoing updates to SGNA and ASGE guidelines reflect a field that continues to evolve. Every endoscopy program needs a named person responsible for tracking regulatory and guideline updates and translating them into policy revisions and staff training, not as a one-time project, but as an ongoing operational commitment.
The endoscopy patients counting on these systems are often among the most vulnerable people in a healthcare facility. They have consented to a procedure in the belief that the systems and standards their healthcare team follows will protect them. Honoring that trust is the ultimate purpose of everything in this guide.
Reprocess with rigor. Train with intention. Audit with honesty. And when in doubt, follow the IFU.
Works Cited
Download Our GI Reprocessing Resource Packet
Your complete clinical resource packet for endoscope reprocessing compliance, training, and best practices. Fill out the form below and we'll send it straight to your inbox.
No spam. Unsubscribe anytime.