Damage Unseen, Infections You Can’t Ignore: Endoscopes and Infection Risks
Ask most reprocessing teams what stands between a patient and an endoscope-related infection, and they’ll point to their protocol: manual cleaning, high-level disinfection, drying, storage. Each step checked, logged, and signed off. In most facilities, that protocol is followed correctly, every time. So why do endoscopes keep testing positive for pathogens anyway?
A growing body of research points to an answer that has little to do with whether staff followed the steps, and everything to do with the physical condition of the channel itself. One study using magnification and borescope inspection found actionable defects that could interfere with reprocessing effectiveness in 100% of the endoscopes examined, with scratches present in 88% of channels, shredding or peeling in 80%, and dents in 40%, all at baseline, before microbiology even entered the picture.¹
That’s the finding at the center of this post: worn and damaged endoscope channels create the physical conditions biofilm needs to take hold, and this damage routinely survives, and defeats, even guideline-compliant reprocessing.
Why this Matters
One academic medical center that implemented a systematic borescope inspection program tracked its endoscope repair costs over three years. Total repair spending fell from roughly $1.21 million to about $724,000, and the average cost per repair dropped by roughly half, from around $4,000 to about $2,000.⁷ The logic is straightforward: catching damage early, before it worsens or forces an emergency out-of-cycle repair, is consistently cheaper than reactive fixes.
Factor in the infection side of the ledger, and the case gets stronger still. Hospital-acquired bloodstream infections, the broad cost category an endoscope-transmitted infection would fall into, cost an estimated $45,814 per case on average, making them among the most expensive infection types tracked nationally.⁹
How Channel Damage Actually Happens
Endoscope channels can become damaged every time they’re used. Instruments, brushes, and forceps pass through narrow, curved lumens during both the procedure and the cleaning that follows, and each pass can abrade the channel’s interior lining. Researchers have hypothesized that this repeated mechanical contact directly drives channel damage, which in turn promotes bacterial attachment and biofilm formation.²
From Scratch to Biofilm: The Microbiology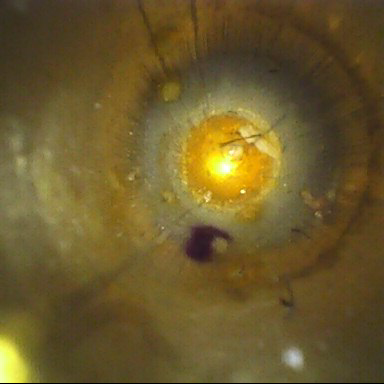
Biofilm is what happens when bacteria stop floating freely and attach to a surface, multiply, and wrap themselves in a self-produced protective layer. Bioburden refers to the total microbial load on a device before decontamination. Rough, damaged surfaces give bacteria more places to grip and hide, which is why channel wear and biofilm formation go hand in hand.
The organisms recovered from damaged channels aren’t hypothetical. One study dislodged biofilm from endoscope channels before culturing them, and found 47% came back culture-positive, including Shigella dysenteriae and resistance-prone organisms like Pseudomonas aeruginosa, Klebsiella pneumoniae, and E. coli.³
Why Damaged Channels Are Harder to Clean
Damaged channels aren’t just more likely to harbor biofilm, they’re harder to clean once biofilm forms. Damage traps bioburden, which demands more aggressive cleaning, which risks causing more damage, a cycle that compounds over the device’s life. Research comparing cleaning approaches found manual cleaning failed to remove biofilm from precisely these channels, flagging this gap as a plausible root cause behind a share of reported endoscopy-associated infections.⁶
What This Means for GI Reprocessing Programs
Improve manual cleaning outcomes directly.
Brushing and flushing deserve special scrutiny. Disinfectants are directly inhibited from effectiveness in improperly cleaned channels. Better technique also means fewer passes and less force during cleaning, which can slow the rate of new channel damage, tying cleaning quality directly back into damage prevention. High-level disinfection or sterilization outcomes are directly dependent on cleaning.
Treat device condition and cleaning technique as inseparable.
A better protocol can’t fully compensate for a damaged channel — and a facility can’t get an honest read on device condition without first knowing its cleaning technique is consistent.
Make inspection routine, not occasional.
Visual and borescope inspection should be a standard part of every reprocessing cycle, not reserved for outbreak investigations. Conduct risk-assessments to identify areas in most need of inspection, and make periodic advancements towards total visual inspection of endoscope inventories. Report when something is found and be systematic about program improvements.
Give damage findings a defined action pathway.
A scratch or visible debris shouldn’t just get logged. It should trigger a decision: repair, retire, or route to enhanced reprocessing.
Verify visual inspection
Today things seen can be further verified with testing such as ATP (adenosine triphosphate) or protein testing. Multi-layered quality assurance programs answer finer, more nuanced questions when problems or breaches in reprocessing arise.
Worn and damaged endoscope channels aren’t a cosmetic detail or a maintenance footnote. They’re a documented, recurring, usage-driven contributor to biofilm formation, which in turn, impacts patient outcomes. Proactive, systemic improvements to both visual inspection and manual cleaning practices work double-duty to strengthen outcomes for patients.
Ready to explore more? Earn 2 free HSPA CE’s reading our Ultimate Guide to Endoscope Reprocessing, and test your knowledge in all things GI!
Citations and Further Readings
- Ofstead CL, Hopkins KM, et al. “Borescope inspection of endoscope working channels: Why and how?” American Journal of Infection Control / PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8759935/
- “Contribution of usage to endoscope working channel damage and bacterial contamination.” American Journal of Infection Control / PubMed. https://pubmed.ncbi.nlm.nih.gov/32169614/
- “Determination of bacterial species present in biofilm contaminating the channels of clinical endoscopes.” ScienceDirect. AECC shows potential to deliver enhanced cleaning over current practice to all endoscope channels and may thereby address infection risk. https://www.sciencedirect.com/science/article/abs/pii/S2468045118300440
- “Inspection of endoscope instrument channels after reprocessing using a prototype borescope.” ScienceDirect / PubMed. https://pubmed.ncbi.nlm.nih.gov/29753038/
- “Borescope examination: Is there value in visual assessment of endoscope channels?” Gastrointestinal Endoscopy (Editorial). https://www.giejournal.org/article/S0016-5107(18)32846-3/fulltext
- “Comparison of two endoscope channel cleaning approaches to remove cyclic build-up biofilm.” ScienceDirect. https://www.sciencedirect.com/science/article/pii/S0195670124001993
- “How Inspecting Borescopes Can Save Money and Lives.” AAMI, reporting on Ofstead CL, et al., “Impact of Borescope Inspection on Endoscope Repair Frequency and Cost,” Biomedical Instrumentation & Technology (2024). https://aami.org/news/below-the-hospital-borescope-inspections-cori-ofstead/
- “The Hidden Cost of Endoscope Damage: A Case for Proactive Repair Programs.” Probo Medical. https://www.probomedical.com/learn/blog/the-hidden-cost-of-endoscope-damage-a-case-for-proactive-repair-programs/
- Zimlichman E, et al. “Health Care–Associated Infections: A Meta-Analysis of Costs and Financial Impact on the US Health Care System.” JAMA Internal Medicine, cited via One Health Trust. https://onehealthtrust.org/publications/infographics/overall-and-unit-costs-five-most-common-hospital-acquired-infections-in-us/