Reprocessing Considerations for 5 of the Most Difficult-to-Clean Surgical Instruments
As surgical procedures advance, so does the complexity of the design and reprocessing methods for devices in both the sterile processing and gastroenterology departments.
Many instructions for use (IFU) that were once short and easy to understand are now rigorous, time intensive, and difficult to measure. This increase in the complexity of IFUs, tied with other environmental challenges such as staffing shortages, changing guidelines, and lack of control over the operating room’s pre-cleaning quality, makes staying compliant with IFUs more difficult than ever.
Certain surgical instrumentation is more challenging to reprocess than others. Here are five types of surgical instruments that may require additional planning and consideration by staff to ensure reprocessing IFUs are being met.
1. Robotic instrumentation

Robotic devices continue to pose reprocessing challenges for sterile processing staff due to their intricate ‘nooks and crannies’ and the inability to be disassembled for cleaning and inspection.
A 2016 Infection Control & Hospital Epidemiology study conducted on cleaning robotic instruments concluded that it is ‘virtually impossible’ to fully remove contamination from their arms.
“These instruments are wonderful tools that allow surgeons to operate with care; but completely decontaminating them has been a challenge for hospitals,” said Yuhei Saito, RN, PHN, MS, lead author of the study and assistant professor at the University of Tokyo Hospital.1
Sterile processing departments may also face another challenge: Robotic arms that are too long for many of their existing sink basins. New process requirements and standards can render current work stations and department designs obsolete and outdated, adding to the challenge of non-compliance. This now presents a need for additional budget considerations to include additional equipment or updated workflow requirements.
Consider the following questions whether you’re evaluating existing robotic practices or just getting started:
- Do my sink basins fit robotic arms for proper soaking?
- Can I sacrifice a sink basin for a full, 30-minute soaking period, per IFU requirements?
- Am I really flushing robotic channels for their full IFU every time, and can I ensure I meet pressure requirements?
- Do I have the automated cleaning systems in place to meet robotic IFUs?
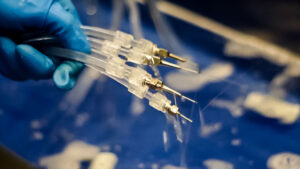
2. Flexible endoscopes
Flexible endoscopes are notoriously difficult to reprocess due to their complex designs. Some of these design elements might include:
- Long, dark, and often narrow channels, which favor bioburden and biofilm development, especially if channels are left wet and/or improperly cleaned
- Elevators
- Rough or pitted surfaces

- Heat and chemical sensitive construction
- Right angle bends, and complex ports
AAMI ST91:2021 section 6 indicates that anyone responsible for reprocessing of flexible endoscopes must go through a formal training plan with a competency evaluation. Certification is also becoming a high priority as the industry strives for consistent and reliable reprocessing practices. Training and continued education takes a front seat in best practice when it comes to flexible endoscope reprocessing Knowing and understanding the complexity in the design and u se of flexible endoscopes helps to eliminate the preventable errors and challenges face in endoscope reprocessing.
3. Ocular and ophthalmic instruments
Any ocular surgery where the anterior segment is exposed is at risk of a potential Toxic Anterior Segment Syndrome (TASS) infection. These procedures not only include cataract cases, but also eye trauma and macular degeneration procedures. Facilities reprocessing instrumentation which supports these cases should pay special attention to ANSI/AAMI ST79:2017 “Comprehensive guide to steam sterilization and sterility assurance in health care facilities” guidance.
Ocular instruments should be processed in dedicated areas of the department solely for eye instrumentation. Eye instrumentation IFUs may, for example, restrict the use of enzymatic detergents. When residual enzymatic gets in a patient’s eye during a procedure, it can lead to blindness or other severe, negative outcomes. You may also find your ocular IFU now includes single-use brushes only, or specific water quality requirements. Review your IFU carefully for these common, unique considerations.
4. Flexible reamers
Loaner instrumentation poses a unique challenge for reprocessing departments. Many staff members may be asked to clean instrumentation for the first time without adequate training and preparation. A lack of communication from vendors on IFUs and proper cleaning protocols could further complicate the cleaning process. Even if the instrumentation is not complex in its design, a lack of education, training, communication and available resources can compromise the quality of consistent and standardized care.
Having a robust loaner instrumentation program, including strict IFU reporting by vendors, a thorough decontamination process for instruments arriving at your facility for the first time, and giving teams proper time to clean pre- and post-procedure can help reduce manual cleaning errors. 3
For any department that is reprocessing any of these complex instrument designs, proper training and processes become foundational to ensuring your patients’ well being and safety.
References
- Yuhei Saito, Hiroshi Yasuhara, Satoshi Murakoshi, Takami Komatsu, Kazuhiko Fukatsu, Yushi Uetera. Challenging Residual Contamination of Instruments for Robotic Surgery in Japan. Infection Control & Hospital Epidemiology, 2016; 1 DOI: 10.1017/ice.2016.249
- Lopes LKO, Costa DM, Tipple AFV, Watanabe E, Castillo RB, Hu H, Deva AK, Vickery K. Complex design of surgical instruments as barrier for cleaning effectiveness, favouring biofilm formation. J Hosp Infect. 2019 Sep;103(1):e53-e60. doi: 10.1016/j.jhin.2018.11.001. Epub 2018 Nov 10. PMID: 30423413.
- Sadler, D. (2016, November 15). Cover story: The challenges associated with loaner instrumentation. OR Today. https://ortoday.com/cover-story-the-challenges-associated-with-loaner-instrumentation/.
RELATED PRODUCTS
